
The Robodebt of Aged Care: MND Reveals that Aged Care and NDIS Are Systems Built to Miss the Point
In November of last year, aged care reforms were implemented in response to the Royal Commission. In the few months since implementation, there has been alarm at how the reforms are impacting on people who are reliant on aged care. In today’s long-read article, Jayne Christian, a Baramadagal Darug woman with a background in the law and cultural arts, shares her lived experience of navigating the aged care system on behalf of her mother, Julie-Ann, who has been diagnosed with motor neurone disease. Jayne has blogged extensively about their ongoing experiences with aged care; you can read more of her writings on this topic here.

Jayne and Julie-Ann Christian. Image credit Joseph Mayers.
Recently, I have spoken publicly about aged care reform failures impacting people living with Motor Neurone Disease (MND), including an appearance on Seven National News at Midday and having our family story printed in the Daily Telegraph. These conversations have been urgent, and are now finally starting to pierce the public conscience.
The system is not failing. It is functioning exactly as designed.
Waanyi and Jaru man, Professor Gregory Phillips, argues that Aboriginal health is fundamentally about power and power relations between Aboriginal people and the state (See for example Phillips, 2015). What is often framed as “inclusion” within systems is, in practice, the maintenance of those power structures. In this context, “care” is not being delivered with people, but is being imposed upon them, often in ways that we see cause harm.
Phillips contends that the Australian public health system itself can contribute to the production of sickness through its reliance on individualising, epidemiological measurement, and rigid planning and governance techniques (Phillips, 2015). (Phillips, 2015). This is not a failure of awareness, but a failure of structure.
Similarly, Mununjali and South Sea Islander woman, Professor Chelsea Watego, reminds us that these systems are not broken, they are operating as intended, continuing to marginalise Aboriginal people who are then expected to navigate that harm rather than be protected from it (Watego, 2021).
Aboriginal scholars have long identified these patterns across health, legal, and welfare systems. The reason it is important to reference Indigenous thinkers from the outset is because Aboriginal and Torres Strait Islander peoples have experienced the failures of every system in this settler-colony that has purported to deliver “care” since colonisation began. From that experience, we know this: when you get things right by Aboriginal and Torres Strait Islander peoples, you leave nobody behind.
The failure of the 1 November 2025 aged care reforms is indiscriminately affecting people. But at its core, what we are witnessing is not new, or an exception, but simply an extension of how government systems have always operated.
Governance structures and their departments and delegates that are capable of dehumanising and causing harm to Aboriginal and Torres Strait Islander peoples are capable of causing harm to anyone. Which is why it is so often Aboriginal and Torres Strait Islander peoples who find ourselves reminding the nation of our shared humanity. Because when respect for our shared humanity is not the baseline - nobody is safe, and nobody knows that on these lands more than us.
No priority even when there is no cure for your disease
Motor neurone disease (MND) is a poorly-understood condition in which the motor neurons – the nerve cells that control the movement of voluntary muscles – progressively weaken and die. With no nerves to activate muscles, people with MND lose their ability to walk, speak, swallow and ultimately breath. It affects each person differently, but there is no cure and it often progresses very rapidly, especially in older people. The clinical and support needs are extreme.
Since the introduction of new reforms, our family has experienced the system in ways that expose its underlying logic.
I registered my Mum with My Aged Care in 2018 after a fall unrelated to MND, at a time when she only needed light assistance, commencing on a Level 2 (see Figure 1 for approximate package values).
Since MND symptoms commenced in 2020 we’ve had to wait for reassessments, approvals and allocation. At no time was our situation genuinely looked at with fresh eyes, instead being made to wait 11 months from approval for an increase to Level 3, to be allocated in October 2025.
In early November 2025, a reassessment that should have increased support beyond Level 3 denied an increase based on an algorithm determination (the “integrated assessment tool” that has been in the media, see here and here). When challenged, it was instead replaced with a decision to approve Level 7, but approval does not mean allocation, we are still waiting without resolving immediate care needs.
On 27 March 2026, a five-month “systems review” disputing the standard wait time, an accurate estimate of 10–11 months, for a person with MND was ultimately dismissed with the delegate affirming that standard wait times should still apply.
Figure 1: Comparison of the defunct Home Care Packages and current Home Support Packages
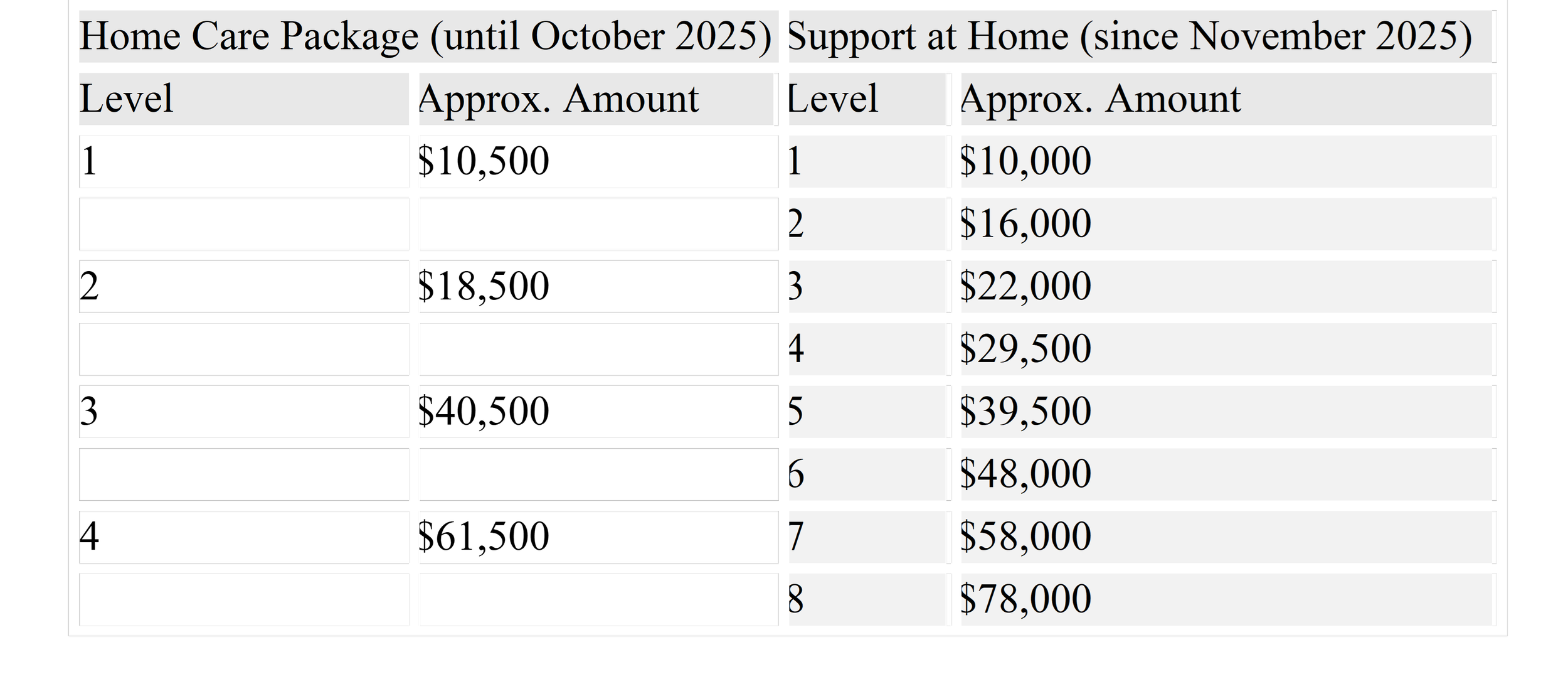
An increase in approval to a Level 8 was also requested by the System Governor as part of the review process, and despite corroborating evidence from treating practitioners, who all concur that the highest level of support (Level 8) from the aged care system is inadequate to support families living with MND, this increase was denied. The level 8 packaging is approximately $200,000 per annum less than families in receipt of NDIS receive for the same condition.
My Mum will never be eligible for NDIS because despite living with MND symptoms three years prior to the NDIS cut off age of 65, she did not receive a diagnosis until 3 years after the NDIS cut off age. While this level of bureaucracy maddens me, I can only give thanks to the higher powers that we are dealing with Primary Lateral Sclerosis (PLS) MND rather than Amyotrophic Lateral Sclerosis (ALS) MND, which carries a typical life expectancy of 27 months from diagnosis.
For additional context, a Level 3 in the now defunct Home Care Package (HCP) system equates to a Level 7 in the newly-introduced Support at Home (SaH) system, if the current approval is ever allocated, the material difference in our annual support would be $17,095.
I’m not sure at what point in this health journey the system would expect me to be providing 24/7 clinical and caring support to my Mum and seek a reassessment for a priority Level 8 again, which would mean having ACAT workers in our home again, to understand our day-to-day life again, providing compelling medical material again, all to be told again that they cannot increase the SaH level because she has not cognitively declined (not a symptom of her MND) and she is not homeless (even if our living arrangement is crisis-driven, because I will not leave her).
This is not a gap in the system, this IS the system. When interviewed by Natarsha Belling, I was asked about the impact of the reforms, and after speaking to a number of media people that day before the interview, it occurred to me that these people were genuinely shocked. What seems to have caught their attention was learning that on a widespread scale older people are having to choose between showers or food. Was that the case for us? I was asked pre-interview.
I said we do not have to choose between those things in the package, because although a package can provide those things, the funding allocated to a Level 3 package does not go far enough to create that choice. My Mum lives with an incurable neurological condition which means I have to shower her, prepare her food and provide constant care. The Level 3 package we get pays for allied health care assessments and reports, two physiotherapy sessions a week and a few hours of housework. Our package doesn’t extend to assistance in the bathroom, the kitchen or even getting the lawn mowed.
Yet we are currently renting a BiPap ventilation machine to assist with my Mum’s breathing overnight. A BiPap machine costs around $5,000, and we are not eligible for the Enable NSW program which covers these costs, because we are deemed to be supported… by a SaH aged care package.
Never having been in receipt of a Centrelink payment, and despite having provided care for some time, I applied for the Carers’ Allowance ($162.60 per fortnight) on 4 December a couple of weeks after receiving Mum’s formal diagnosis. I thought I could at least put this toward her care in the absence of adequate aged care funding, and because as at the time I was paying for the physiotherapy sessions because the business providing the package was not convinced she was in need of that service, interestingly they didn’t need convincing to provide housework services which they benefited from providing. We now self-manage and over four months have passed and I am still waiting for that Carers’ Allowance application to be processed.
In the absence of medically informed processes - bureaucratic escalation becomes the only pathway
It became apparent during the Department of Health, Ageing and Disability’s internal Systems Governor review process, that it is a flow-chart style decision making process: rigid, procedural, and largely void of empathy, discretion, or comprehension of medical reality. Points can only be awarded for predefined categories. We were not awarded points for “homelessness” because I am sustaining my Mum’s less-than-ideal living situation, nor for “cognitive decline,” because, despite my Mum being an Aboriginal woman living with a life-limiting, non-curable illness, her cognitive function is good. On that basis, our need and urgency were not recognised.
Similarly, shortly prior to Easter, Darren Chester MP spoke in Parliament about constituents who had reached out to him, including a couple who were 99-year-olds needing immediate support to remain at home, yet were told they would need to wait approximately 12 months for services, as their situation was not considered “urgent” because they were not Indigenous, homeless, or experiencing cognitive decline.
This reflects a broader government dynamic that divides and categorises people in ways that produce both exclusion and resentment. It reinforces harmful stereotypes, including the persistent myth that “Aboriginal people get everything for free”, while simultaneously conditioning non-Indigenous people to believe they must present in particular ways to access care they need.
At the 2025 Indigenous Wellbeing Conference held on Jagera and Turrbal Country (Meanjin / Magandjin / Brisbane), Professor James Ward opened his keynote with a confronting statistic: between the 2016 and 2021 Census, there was an increase of 83,000 people identifying as Aboriginal or Torres Strait Islander peoples, after accounting for births and deaths. While these trends place additional pressure on already stretched communities, they must also be understood in the context of the broader political and administrative environment - one in which access to services is mediated through systems that reward categorisation instead of responding to need.
At the current time, I have:
Lodged an Aged Care Quality Complaints Commission complaint against a previous package provider for breaching a rule in the Support at Home program manual i.e. passing on a charge to my Mum that Services Australia refused to pay, and admitting that to me in writing. It was dismissed this week by the ACQCC because the provider refused to answer their questions or reimburse the funds.
Lodged an Administrative Review Tribunal appeal to the decision not to increase funding level or allocation priority.
Submitted a complaint to the Commonwealth Ombudsman regarding the negligent decision making of Department of Health, Ageing and Disability.
Made a submission to the UN Special Rapporteur ahead of their 2026 visit. In that submission, I stated without doubt that the aged care system is operating in ways that serve settler-colonial objectives, and, in doing so, it is a mechanism in the erasure of older Aboriginal people living with disability.

Julie-Ann sitting under a tree that she advocated for (successfully) to be heritage listed. Image credit Jayne Christian.
What “care” looks like when the system doesn’t show up
In another piece, I wrote about “true respite.” To us it means getting to be in our own home or on our own Country without feeling like we are on other people’s to-do lists, without being harassed by phone calls, or having to repeatedly explain medical and practical reality and urgency to those who cannot hear us from inside their bureaucratic bubbles.
I did not know until I tried to arrange a short-term, two-week respite for the first time, that it would be difficult to secure because aged care centres are buckling under the weight of permanent placement waitlists. I was not aware that aged care homes are struggling to place a backlog of around 5,000 older people who are in hospital beds, some being placed in homes now after waiting almost three years in hospital. Many aged care homes cannot handle residents with complex needs.
Right now, care is nowhere in sight in the aged care system. It is being absorbed by families, unpaid, unsupported and when they cannot or will not continue, it is being left to the public health system - hospitals. I have also read a number of accounts in recent months of those needing MND care opting for voluntary assisted dying once their carers burn out, if not meeting an undignified end first, due to these abject policy failures.
More packages, less care even with “Care Partners”
A key narrative of reform has been that more packages are being delivered.
But more packages do not automatically mean more care, or the level of care required. Without flexibility, responsiveness and discretion, increased funding can still produce the same outcome:
services that do not meet need;
delays that do not respond to rapid decline; and
a system that measures outputs rather than impact.
In 2025, my Mum’s Care Partner responded to our needs and covered a broad range of supports under a Level 2 package, including domestic assistance, personal care, garden maintenance and physiotherapy. However, while packages are structured to cover multiple services, the funding itself is insufficient to meet actual need.
Once the package funds were depleted, we were left with no support while it replenished over approximately five months, during which time my Mum’s condition continued to decline and I was left to manage alone.
In response, I transferred to another Care Partner. They would only agree to fund one physiotherapy session per week, meaning I paid for the second session myself. They then introduced a policy requiring providers to hold cyber security insurance and refused to pay for either session until the physiotherapist obtained cyber security insurance specifically. Our physiotherapist’s broker advised this was not relevant to his practice and would impose unnecessary cost. Despite this, the Care Partner insisted, suggesting it was linked to the 1 November reforms, when in reality it was an internal policy decision. As a result, I was forced to cover both physiotherapy sessions at $160 each, or $320 per week until we changed provider.
In January, I moved to a self-managed arrangement with a different Care Partner. Prior to signing, we were told we could choose our own workers from any platform. Prior to booking a specific worker we checked the specifics with them and it was reiterated that there would be no issue with them paying the worker we’d selected. After onboarding, this changed. They refuse to pay the domestic assistance worker, someone with whom we have built trust and rapport, and instead directed us to use workers from their own platform.
As it stands, my Mum’s package now covers two physiotherapy sessions per week, but not the home care worker we have chosen to retain. I pay for that support out of my own pocket. At the standard rate, 2.5 hours of assistance costs $172.73, and on a public holiday the same service costs $390.08.
This is where we must know the behaviours and bottom lines of a community versus an economy, and we must remember the worth of our Old People from a place of knowing grounded in our full humanity, not from a world where AI algorithms and bureaucrats in denial have redefined what that means and looks like in our daily lives.
Why this is not surprising
As a Baramadagal woman, none of this is surprising. I retired at age 36 from government employment, due to racism, racism-denial and garden-variety bureaucratic saturation. That same year coincided with my Mum and I realising that she might have a serious neurological condition - but only time would tell.
Decision-makers are operating within bureaucratic structures that are inherently disconnected from community and the realities of lived experience.
They are trained to maintain the status quo, which means prioritising administrative order over human urgency. Consistency in this context, though, means applying the same timelines to people whose conditions are running on fundamentally different timelines. It is treating MND like ordinary ageing, when it is not.
What becomes clear is that many decision-makers are not malicious. They are operating within systems that have shaped how they see the world. But those systems and worldviews create distance, and in that distance harm is normalised, and inflicted en mass.
What needs to change
If aged care reform is to mean anything, it must return to humanity-centred approaches, which means local place-based community services that genuinely care and listen to people about what is needed from their packages and be able to respond to that need without restrictive red tape. There can be no place for business models like we see now, commodifying the ageing process, in community care.
As a matter of priority, specifically to MND:
The Federal Government must implement the five key policy initiatives set out by MND Australia:
These initiatives focus on:
o Linking MND data for national impact
o Increasing access to quality specialist care and research
o Fast-tracking Aged Care for people living with MND
o Funding disability supports in Aged Care at a comparable level to the NDIS
o Protecting future generations through genetic testing and counselling
The State Government must increase funding for both MND NSW and for strengthening MND Clinic cover across the state.
We must be louder than the silence of departmental denial
Sam Rae’s (Minister for Aged Care and Seniors) office spent $215,168.89 between October and December 2025 in expenditures. In addition, based on standard ministerial remuneration, he would be earning approximately $6,300 to $6,700 per week before tax. Against this backdrop, it raises serious questions about accountability when those responsible for the system are so far removed from the conditions experienced by those relying on it.
What MND is revealing is the limits of a system that was never designed to respond to nuance, complexity and urgency. For Aboriginal families in particular, these failures compound and sit within a longer history of systems that:
wilfully misunderstand
continue to exclude
and ultimately erase
The question is not whether the system is working. It is: who is it working for?
Because for families like mine, and for many others seeking assistance during the ageing process and living with conditions like MND, the answer is increasingly clear. It isn’t working for us.
And unless something shifts, not just in how policy decisions are made, but in how people and communities are valued - then it simply won’t.
References
Greg Phillips, Dancing With Power: Aboriginal Health, Cultural Safety and Medical Education (PhD thesis, 2015), and related work on cultural safety, power, and institutional accountability
Chelsea Watego, Another Day in the Colony (2021)
Christian, J. (2026), The Robodebt of Aged Care is Already Here; True Respite; Christmas is Coming Faster than Priority Care for MND; An Update: Aged Care, MND in the Riverina and Bureaucracy; Aged Care Price Hikes Aren’t the Shock MSM Make Them Out to Be; More Packages, Less Care: How Reform Missed the Point
Content moderator: Sue Olney